Charge Capture in Healthcare Revenue Cycle Management
Charge capture in healthcare ensures all services are billed correctly. It plays a key role in improving revenue cycle management, reducing claim errors, and maximizing reimbursements.
April 17, 2026


Key Takeaways:
• Charge capture is the process of documenting all billable services, procedures, and supplies provided during a patient encounter—before coding or billing begins. In the RCM workflow, it's the critical handoff point between care being delivered and a claim being built.
• HFMA reports hospitals lose as much as 1% of net patient revenue to charge capture issues. For a $200M hospital, that's $2 million in services delivered but never billed.
• The most common errors are missed charges, charge lag, erroneous charges, chargemaster mismatches, and undercoded E&M visits.
• Capturing charges is only half the battle—accurate coding and clean claim generation downstream determine whether those charges actually become revenue.
Healthcare providers lose more revenue to charge capture errors than most realize.
Not through significant billing failures, but through the quiet accumulation of small misses—a service going undocumented, a complexity level understated, a supply used but never recorded, and so on.
According to HFMA, hospitals lose as much as 1% of their potential annual net revenue to charge capture issues alone. For a large hospital, that's easily $1-2 million walking out the door every year.
Getting the charge capture process right starts with understanding exactly where it fits, where it breaks, and practical ways to fix it. This guide covers all of it.
On this page
- What is Charge Capture?
- Where Does Charge Capture Fit in the Revenue Cycle?
- Charge Capture vs. Charge Entry: What's the Difference?
- Is Charge Capture the Same as Clinical Documentation?
- How the Charge Capture Process Works (Step by Step)
- Common Charge Capture Errors and What They Cost
- How to Improve Charge Capture Efficiency
- Strengthen Your Charge Capture Process
- FAQs
What is Charge Capture?
Charge capture is the process of documenting all billable services, procedures, and supplies provided during a patient encounter so they can be accurately coded and billed.
This involves recoding encounter details like:
- Every procedure performed
- Every supply used
- Every minute of provider time spent with a patient
This documentation typically happens at or right after the point of care: either during charting or immediately after the patient leaves.
If a billable service isn’t captured at this stage, it won’t be coded, creating a ripple effect where it ultimately isn’t coded, billed, and paid.
Components of Charge Capture
Charge capture covers:
- Evaluation and management (E&M) visits—office visits, consultations, hospital admissions
- Procedures and surgeries—from minor interventions to complex OR cases
- Diagnostic tests— lab work, imaging, pathology
- Medical supplies—bandages, catheters, infusion materials, implants
- Medications administered—particularly in hospital and infusion settings
- Ancillary services—physical therapy, respiratory therapy, social work consultations
What it does not cover is the translation of those services into standardized billing codes (that's coding) or the entry of those codes into billing software (that's charge entry). We’ll cover more on those distinctions shortly.
Where Does Charge Capture Fit in the Revenue Cycle?
Charge capture sits in the mid-cycle of the revenue cycle. The image below shows how the full RCM workflow breaks down into three phases:
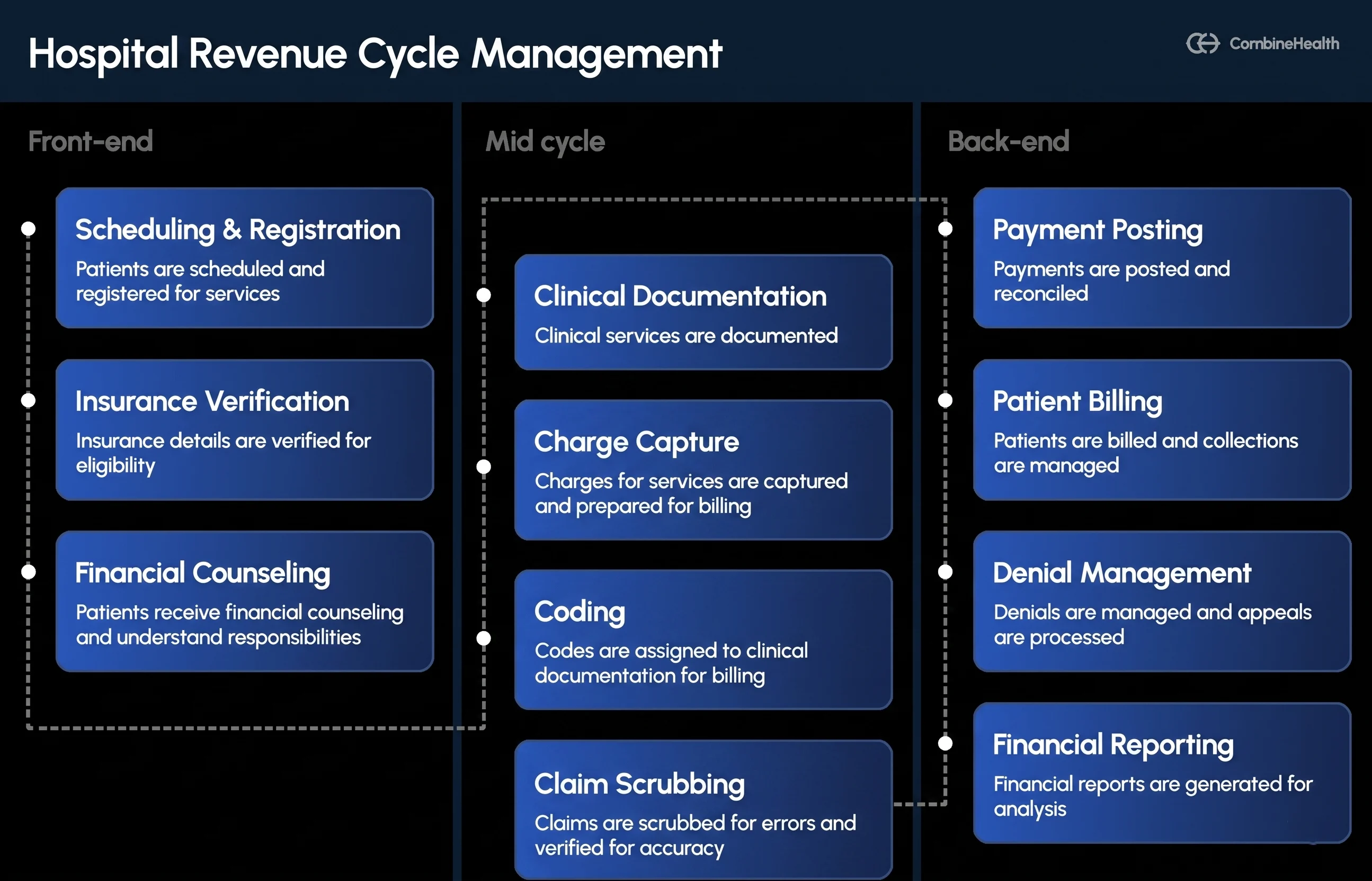
- The front-end handles patient scheduling, insurance verification, and financial counseling.
- The back-end covers payment posting, patient billing, denial management, and reporting.
- Charge capture lives in the middle—right where clinical activity gets translated into billable charges.
Its position matters. Everything upstream (documentation quality, insurance verification) determines whether charge capture has what it needs.
Everything downstream (claim scrubbing, submission, payment) depends on whether charge capture was complete and accurate. If services aren't captured here, they don't exist in the rest of the revenue cycle management pipeline.
Charge Capture vs. Charge Entry: What's the Difference?
Charge capture and charge entry are two distinct steps in the billing workflow—performed by different people, at different times, using different tools.
Here’s how the above difference plays in practice:
A physician documenting each patient encounter in the EHR (recording the services performed, supplies used, and clinical details) is charge capture.
A billing specialist later reviewing those documented encounters, assigning the correct fee schedule amounts, and entering them into the practice management system—that's charge entry.
Both steps are critical to accurate medical billing. But they fail in different ways and require different solutions.
- Charge capture fails when services go undocumented
- Charge entry fails when documentation is correct but entered incorrectly or incompletely.
Is Charge Capture the Same as Clinical Documentation?
No, charge capture and clinical documentation are not the same. Though they're closely connected.
Clinical documentation is the comprehensive medical record of a patient encounter. It captures the full clinical picture: symptoms, diagnoses, treatment plans, provider notes, and test results. Its primary purpose is to support continuity of care, legal accountability, and compliance.
Charge capture pulls the billable layer from that clinical record. It asks a narrower question: which services were rendered that can be submitted to a payer for reimbursement? Every procedure, supply, and encounter that belongs on a claim starts here.
The two processes overlap heavily—especially when charge capture is embedded directly in the EHR workflow. But a provider can write thorough, detailed clinical notes and still have poor charge capture if the billable items aren't explicitly flagged for the billing team.
That gap between what's documented clinically and what's actually captured for billing is one of the most common sources of revenue leakage in healthcare.
Recommended reading: A guide to Clinical Documentation Improvement (CDI)
How the Charge Capture Process Works (Step by Step)
Charge capture is not a one-step task. It's a mini-workflow that involves both clinical and administrative staff, running parallel to patient care.
Here's how the process typically moves:
Step 1: Service Delivery
The provider sees the patient and delivers care. Procedures are performed, supplies are used, and medications are administered. This is the moment charges are generated—even if they aren't captured yet.
Step 2: Documentation at the Point of Care
As care is delivered (or immediately after), the provider or clinical staff documents what was done. Every service must be recorded with enough specificity to support coding: what procedure, what diagnosis, what site, what level of complexity. In many practices, this information is captured on a superbill.
This is where most charge capture breakdowns begin. Rushed documentation, vague notes, and end-of-shift catch-up charting all create gaps that become missed or unsupported charges downstream.
Step 3: Charge Review and Reconciliation
Before charges move to coding, a designated charge capture specialist or billing coordinator reviews the documented services against the patient's record. This is to ensure everything that was done is reflected in the charge list. This is also where duplicate entries get caught.
Many organizations run a daily or per-shift reconciliation, comparing provider activity logs (procedures performed, patients seen) against charges submitted. Discrepancies trigger a review.
Step 4: Handoff to Coding
Once reconciled, the charge list moves to the coding team. Coders review the clinical documentation supporting each charge and assign the appropriate CPT, ICD-10, and HCPCS codes.
Coding requires charge capture to be complete first—coders can only work with what's been documented. Regular coding audits help ensure this handoff stays clean and nothing billable gets lost in translation.
Step 5: Final Reconciliation
After coding, a final check verifies that every charge has a valid code, every code has sufficient clinical documentation to support it, and nothing was dropped in the handoff. This is the last gate before charge entry begins.
Common Charge Capture Errors and What They Cost
Charge capture errors are almost inevitable—even in well-run organizations. The goal is to catch the errors before they affect revenue.
Here are the most common ones:
The financial impact of these charge-capturing errors builds up fast. As cited by HFMA, Novant Health, a 14-hospital system with $4.3 billion in annual net patient revenue, uncovered $7.5 million in recoverable revenue in just 15 months after overhauling its charge capture process—from charges that had been missed, miscoded, or never submitted.
How to Improve Charge Capture Efficiency
1. Standardize Documentation at the Point of Care
Inconsistency in how providers document services is the root cause of most charge capture problems.
Implement structured templates in your EHR for common encounter types—ones that prompt providers to document every billable element before closing a chart. Role-specific documentation guides (one for physicians, one for nursing staff, one for OR teams) reduce the ambiguity.
2. Reduce Charge Lag with Real-time Capture Tools
The longer the gap between service delivery and documentation, the more gets forgotten.
Real-time charge capture tools allow providers to log charges at the bedside or immediately post-encounter, before the detail fades. The goal is to ensure no charge sits undocumented for more than 24 hours.
3. Conduct Regular Charge Capture Audits
Periodic audits—comparing clinical activity reports against submitted charges—surface patterns that aren't visible in daily workflows.
It could help identify service lines that consistently under-capture, providers with high charge lag rates, procedures that are routinely missed, etc. Pairing charge capture audits with regular medical coding audits gives you visibility into both sides of the handoff.
4. Train Clinical Staff
Charge capture is a clinical responsibility as much as an administrative one.
Providers who understand the downstream impact of their documentation make better choices at the point of care. Brief, role-specific training sessions—covering what's billable, documentation requirements, and common errors—consistently improve capture rates.
5. Track the Right Metrics
You can't manage what you don't measure. Some of the key charge capture metrics every RCM team should monitor include:
- Charge lag—target: ≤3 days from service to charge entry (source: HFMA)
- Days not final coded (DNFC)—target: ≤3 days from service or discharge (source: ConiferHealth)
- Denial rate attributable to charge errors—target: <5% of total denials
Tracking these alongside your broader revenue cycle management metrics gives you a complete picture of where revenue is leaking and why.
6. Ensure Accurate Coding and Billing Once Charges Are Captured
Capturing the charge is only the first half of the problem. Even a perfect charge list becomes a revenue leak if the coding that follows it is inaccurate.
Undercoded E&M visits, missing modifiers, incorrect ICD-10 sequencing—these errors happen after charge capture, but they undo its value just as surely as a missed charge would.
Manually reviewing every chart for coding accuracy, applying payer-specific billing rules, and scrubbing claims before submission is time-intensive. And at high volumes, error rates climb no matter how experienced the team is.
This is where CombineHealth's AI agents step in.
- Amy (AI medical coding solution) reads the full encounter record from the EHR, assigns accurate CPT, ICD-10, and E&M codes, flags documentation gaps that could cause denials, and provides a line-by-line rationale for every coding decision. She processes charts with 99.2%+ accuracy and handles high volumes in parallel, so coding doesn't become the bottleneck that charge capture fixed.
- Mark (AI medical billing solution) takes Amy's coded charges, applies payer-specific billing rules, scrubs the claim for errors, and submits it through 50+ payer portals. He also reads ERAs and EOBs to post payments and flag discrepancies—closing the loop between what was captured and what was actually reimbursed.
Together, Amy and Mark ensure the work done in charge capture doesn't get lost in the steps that follow it.
Strengthen Your Charge Capture Process
Charge capture will never be perfect—the pace of clinical workflows makes that unrealistic. But the gap between where most organizations are and where they should be is closable.
Standardized documentation, real-time capture tools, regular audits, and targeted provider training address the most common failure points. The benchmark is a 95%+ capture rate, and reaching it is a matter of process discipline and consistency.
What can make the biggest difference is ensuring the work doesn't stop there. Capturing charges accurately only creates value when the coding and billing that follows is equally precise. That's the gap that CombineHealth's Amy and Mark were built to close.
FAQs
1. What Is Charge Capture in Medical Billing?
Charge capture in medical billing is the process of documenting all billable services, procedures, and supplies provided during a patient encounter so they can be coded and submitted to payers for reimbursement. It occurs right after care is delivered, before coding or claim generation begins.
2. What Is the Difference Between Charge Capture and Charge Entry?
Charge capture is the documentation of what services were provided—typically done by clinical staff at or right after the point of care. Charge entry is the subsequent step, where billing staff input those documented services into the billing system with the correct fee values and codes.
3. What Is the Difference Between Charge Capture and Coding?
Charge capture documents what services were provided. Coding translates those documented services into standardized billing codes (CPT, ICD-10, HCPCS). Charge capture happens at or near the point of care by providers. Coding happens afterward by certified medical coders. Both are essential, but charge capture must be complete before coding can begin.
Recommended Reads







Related Posts
Lorem ipsum dolor sit amet, consectetur adipiscing elit. Suspendisse varius enim in eros elementum tristique. Duis cursus, mi quis viverra ornare, eros dolor interdum nulla, ut commodo diam libero vitae erat. Aenean faucibus nibh et justo cursus id rutrum lorem imperdiet. Nunc ut sem vitae risus tristique posuere.
Explore Our
AI Workforce






Subscribe to newsletter - The RCM Pulse
Trusted by 200+ experts. Subscribe for curated AI and RCM insights delivered to your inbox

Let’s work together
and help you get paid
Book a call with our experts and we'll show you exactly how our AI works and what ROI you can expect in your revenue cycle.