HCPCS Codes vs CPT: Key Differences Every Coder Should Know in 2026
Learn the key differences between CPT and HCPCS codes in medical billing, when both are used together, common coding mistakes, and how accurate coding helps prevent claim denials.
May 26, 2026

Key Takeaways
• CPT covers what a provider does, HCPCS covers what a patient receives. Getting that distinction wrong on a Medicare or Medicaid claim is one of the fastest ways to a denial.
• Both code sets update on different schedules—CPT once a year, HCPCS Level II every quarter. A code valid in code can get rejected if your team isn't tracking both.
• Most drug administration, DME, and orthotics claims need codes from both systems on the same claim.
• At high claim volumes, manual review can't reliably catch every CPT-HCPCS pairing error. AI coding tools apply current code-set rules on every claim, every time.
Staying current with CPT and HCPCS is one of the hardest parts of medical billing.
In 2026 alone, the American Medical Association released 418 changes to the CPT code set—288 new codes, 84 deletions, and 46 revisions. The Centers for Medicare & Medicaid Services updates HCPCS Level II four times a year on top of that.
For coders applying both code sets to real claims, staying current is one of the harder parts of the job.
In this guide, we'll cover everything you need to know about HCPCS codes vs CPT: what each system covers, what changed in 2026, when you need codes from both on a single claim, and the CPT vs HCPCS codes differences that matter most for a clean reimbursement.
CPT stands for Current Procedural Terminology and is developed and maintained by the American Medical Association (AMA).
HCPCS stands for Healthcare Common Procedure Coding System (pronounced "hick-picks"). They’re developed by the CMS.
On this page
- What is a CPT Code?
- What Is an HCPCS Code?
- When Do We Use Both CPT and HCPCS Codes?
- Key Differences Between HCPCS and CPT Codes
- CPT and HCPCS Code Updates in 2025 and 2026
- Common Coding Errors at the CPT-HCPCS Boundary
- How AI Helps with CPT and HCPCS Coding Mistakes
- Cut CPT-HCPCS Coding Denials with AI Medical Coding
- FAQs
What is a CPT Code?
A CPT Code is a standardized five-digit numeric code used to describe the medical, surgical, and diagnostic services performed by healthcare providers.
Every time a physician evaluates a patient, performs a procedure, reads an imaging study, or runs a lab test, that service gets a CPT code. The code communicates to the payer exactly what was done, standardized and consistent across every payer and provider in the country.
CPT codes update annually; coders working from a slightly outdated set risk automatic denials on every affected code.
CPT Code Categories
CPT codes fall into three categories:
CPT Code Modifiers
CPT code modifiers are two-character add-ons that tell the payer something extra about a procedure. They don't change what the CPT code means. They change how it's interpreted.
A few examples of modifiers you'll see often:
- Modifier 25: a separate E/M service on the same day as another procedure
- Modifier 59: a separately identifiable procedure
- Modifier 95: telehealth
A correctly chosen CPT code can still be denied if the modifier is wrong or missing.
Recommended reading: A complete guide to modifiers in medical billing
What Is an HCPCS Code?
An HCPCS code is a standardized alphanumeric code healthcare providers use to bill for products, supplies, equipment, and non-physician services to Medicare and Medicaid.
HCPCS Level I vs. Level II Codes
HCPCS Level I codes are identical to CPT codes—same five-digit numeric format, same descriptions, maintained by the AMA. When a physician service is billed to Medicare or Medicaid, the CPT code submitted is also the HCPCS Level I code. The two are interchangeable in practice.
HCPCS Level II codes are what most people mean when they say "HCPCS”. These are alphanumeric—one letter followed by four digits—and cover everything CPT doesn't.
Maintained by CMS, HCPCS level II codes are mostly used for:
- Durable medical equipment (DME): wheelchairs, CPAP devices, walkers
- Injectable and infused drugs: chemotherapy agents, insulin, biologicals
- Orthotics and prosthetics: knee braces, limb prostheses
- Ambulance and transportation services
- Medical supplies: catheters, surgical dressings
Note: Level III codes were previously used by state Medicaid agencies and Medicare contractors for local billing purposes, but were discontinued on December 31, 2003, to standardize coding nationally under HIPAA.
When Do We Use Both CPT and HCPCS Codes?
On most paired claims, three pieces have to line up:
- The diagnosis (ICD-10)
- The service (CPT)
- The supporting resource (HCPCS)
Examples of CPT and HCPCS Codes Used Together
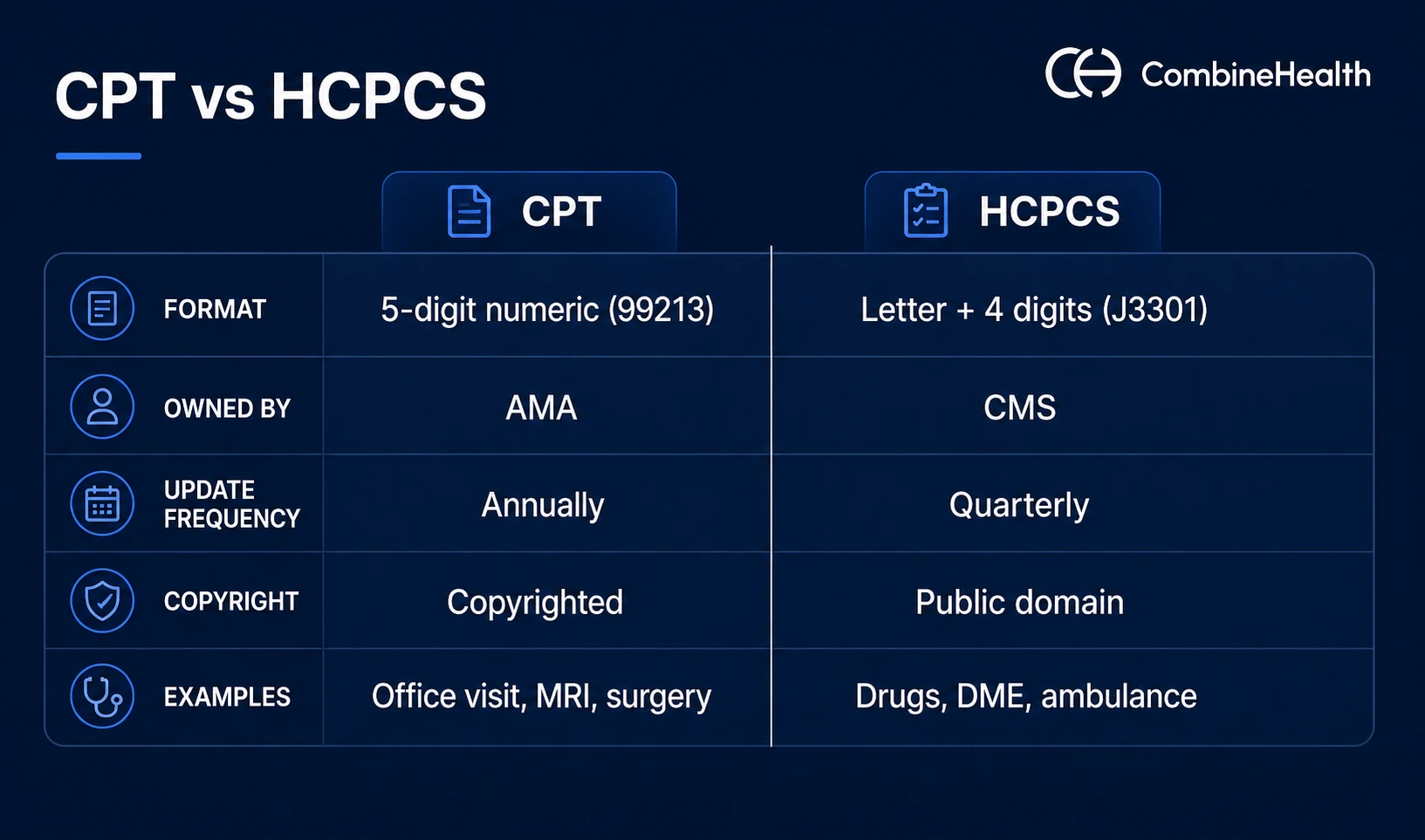
Key Differences Between HCPCS and CPT Codes
CPT describes the services performed; HCPCS describes the drugs, supplies, and equipment used.
Example:
When a provider gives a therapeutic injection, the act of giving it is CPT 96372. The drug itself, say, Kenalog, is HCPCS J3301. Both are needed in the claim for reimbursement.
Without CPT, the payer doesn't know an injection happened. Without HCPCS, they don't know what was injected.
When to Use CPT Codes Vs HCPCS
Start with a simple question: Is this a service or a supply?
If it's a service a provider performed, go for CPT. But, if it's a drug administered, a device dispensed, or equipment sent home with the patient, reach for HCPCS Level II. When it's both, which it often is, you need both codes.
Denial Risk by Code Set
Errors on CPT codes typically trigger medical necessity or documentation denials.
Errors on HCPCS Level II, such as wrong J-code, missing modifier, outdated DME code, tend to result in zero payment on the product or drug line while the service line pays. The revenue leakage from HCPCS errors is often invisible until an AR audit surfaces it.
Update Frequency
CPT updates once a year, effective January 1. HCPCS Level II updates every quarter: January, April, July, and October. Both schedules need to be tracked independently.
Modifiers
CPT modifiers are numeric—25, 59, 95.
HCPCS Level II modifiers are alphanumeric—RT and LT for laterality, JW for drug waste, NU for purchased new, RR for rented. Using a CPT modifier where a HCPCS modifier is required, or omitting one entirely, is a direct path to a denial.
Copyright
CPT is copyrighted by the AMA—access requires a paid license. HCPCS Level II is in the public domain and available free through CMS.
CPT and HCPCS Code Updates in 2025 and 2026
The AMA released the CPT 2026 code set with 418 total changes—288 new codes, 84 deletions, and 46 revisions. All took effect on January 1, 2026. The biggest changes fall into four areas:
The biggest changes fall into four areas:
Remote patient monitoring (RPM)
Five new codes report monitoring services for shorter durations of 2–15 days within a 30-day window. Two more codes report treatment management starting at 10 minutes of clinical staff time per calendar month, down from the previous 20-minute threshold.
AI and augmented intelligence
When a doctor orders a scan, AI now helps read the results, and the AMA added new CPT codes to bill that AI work. Some codes cover AI that spots findings (atrial fibrillation in ECG); others cover AI that measures data (plaque severity on CT).
Hearing device services
Twelve new codes reflect a more patient-centered approach to hearing-aid services. They cover assessing patients' visual, dexterity, and psychosocial factors; validating device performance and sound quality; and training patients to connect personal devices like smartphones to their hearing aids.
Leg revascularization
A full rebuild of the lower extremity revascularization section. The AMA deleted the previous codes and added 46 new ones, reflecting the shift toward outpatient care delivery and expanding access to therapies for patients with persistent leg pain or cramping.
Common Coding Errors at the CPT-HCPCS Boundary
Here’s a handful of common mistakes that drive most denials at the CPT-HCPCS boundary:
- Billing CPT 96372 without a J-code for the drug. The single most common drug-administration denial. The admin code without a matching drug code reads as incomplete.
- DME visits with no HCPCS code. A provider documents a knee brace fitting under an E/M code, but no L-code for the device. The brace cost gets eaten by the practice.
- Reusing last quarter's HCPCS codes. Coders who kept billing S0013 after CMS replaced it with J0013 in Q1 2026 saw clean rejections. Payers don't auto-adjust outdated claims.
- Missing or wrong modifiers. Modifier 25 and 59 often get dropped from claims that pair a CPT E/M with a HCPCS-billed procedure or supply. That leads to bundling denials.
- Mismatched units on J-codes. J-codes are unit-based. For example, "per 10 mg." Bill the wrong units, and you're either underpaid or flagged for upcoding.
| Recommended reading: How to Appeal an Insurance Claim Denial
How AI Helps with CPT and HCPCS Coding Mistakes
Medical coding is one of the highest-volume, most rules-driven workflows in healthcare. That makes it a strong fit for AI, and AI medical coding solutions have become standard for catching the kinds of pairing errors that drive most CPT-HCPCS denials.
The tools read encounter notes the way a coder would, apply current code-set rules, and flag mismatches before claims go out.
How Amy Handles CPT and HCPCS Together
Amy, CombineHealth's AI medical coding solution, reads encounter notes directly from the EHR and assigns ICD-10, CPT, HCPCS Level II, E/M, modifier, and HCC codes in one pass.
For the CPT-HCPCS boundary specifically, Amy:
- Validates that every CPT code requiring a paired drug or supply has the matching HCPCS code attached before the claim leaves the EHR.
- Flags clinical documentation gaps, such as incomplete procedure details, missing findings from independent interpretation, before they become denials
- Provides line-by-line rationale and evidence behind every coding decision, so coders can review and approve quickly
- Audits pre-coded charts to surface systemic coding issues a team might be missing
Trained on more than 1 million medical documents and 100,000+ policy documents, Amy is 99.2% accurate.

Cut CPT-HCPCS Coding Denials with AI Medical Coding
CPT and HCPCS will keep changing on different schedules.
Manual review can keep up, but only if every coder on the team stays current—which is difficult when the AMA pushes 418 CPT changes a year, CMS updates HCPCS every quarter, and every payer has its own pairing rules.
Amy, CombineHealth's AI medical coding agent, automates that heavy lifting. She reads encounter notes from the EHR, assigns correct CPT, HCPCS, ICD-10, E/M, and modifier codes in one pass, and applies payer-specific pairing rules before claims go out.
Book a demo to see how Amy helps your team catch CPT-HCPCS pairing errors before they become denials!
FAQs
1. What is the main difference between HCPCS and CPT codes?
CPT codes describe physician services and clinical procedures. HCPCS Level II codes cover what CPT doesn't, such as durable medical equipment, injectable drugs, ambulance services, and orthotics. Both are used in medical billing, but for different categories of care.
2. Can a single claim contain both CPT and HCPCS codes?
Yes, and many should. Drug administration, DME provision, ambulance transport tied to a visit, and orthotics or prosthetics fitted in-office all typically need a CPT code for the service and a HCPCS code for the supply or drug on the same claim.
3. How do I tell a CPT code from an HCPCS code at a glance?
By the format. CPT codes are five digits, all numeric (like 99213 or 96372). HCPCS Level II codes start with a letter followed by four digits (like J3301 or E0260). The exceptions on the CPT side: Category III codes end with a "T" (0042T) and Category II codes end with an "F" (4011F).
4. Do commercial insurance plans accept HCPCS codes?
Most commercial payers accept HCPCS Level II codes, especially for drugs, DME, and supplies. The catch: some plans use S-codes (an HCPCS subset created for private payers) that Medicare doesn't recognize, and others maintain their own preferred-product lists. So it’s best to check the specific payer's policy before submitting.
Recommended Reads







Related Posts
Lorem ipsum dolor sit amet, consectetur adipiscing elit. Suspendisse varius enim in eros elementum tristique. Duis cursus, mi quis viverra ornare, eros dolor interdum nulla, ut commodo diam libero vitae erat. Aenean faucibus nibh et justo cursus id rutrum lorem imperdiet. Nunc ut sem vitae risus tristique posuere.








Subscribe to newsletter - The RCM Pulse
Trusted by 200+ experts. Subscribe for curated AI and RCM insights delivered to your inbox
Let’s work together and help you get paid
Book a call with our experts and we'll show you exactly how our AI works and what ROI you can expect in your revenue cycle.
Email: info@combinehealth.ai

