ProFee Coding in 2026: The Complete Guide for Maximum Reimbursement
Learn what profee coding is, how it differs from facility coding, 2026 PFS guideline changes, specialty examples, and common mistakes to avoid
May 15, 2026


Key Takeaways
• ProFee coding translates a physician's clinical work into CPT, ICD-10-CM, and HCPCS codes on a CMS-1500 claim—distinct from the facility's UB-04 claim that captures room, equipment, and nursing resources.
• The CY 2026 MPFS final rule introduced two separate conversion factors: a -2.5% efficiency adjustment on non-time-based services, and a 50% indirect PE cut in facility settings—site of service now meaningfully affects what each CPT code pays.
• The most expensive profee mistakes are E/M undercoding, missing modifier 26 on split-billing claims, modifier 25 errors, global surgery package violations, and silent payer downcoding—all invisible without active monitoring.
• Agentic AI now handles profee claims by reading the full encounter, validating against payer policy, and routing only edge cases to human coders for review—shifting the workflow from manual-first to AI-first.
CMS's FY 2025 CERT audit found an 8.4% error rate on Medicare Part B physician claims—i.e., profee claims. If you add payer audits and downcoding, the real losses run much higher.
And in 2026, the rules got tighter.
New CMS rules, updated conversion factors, and permanent telehealth policies have changed how profee services are documented, coded, and reimbursed—and most practices haven't fully caught up yet.
This guide covers the full picture: what profee coding is, how it compares to facility coding, what changed in 2026, how it plays out across healthcare specialties, and where most practices bleed revenue without knowing it.
On this page
- What Is ProFee Coding?
- ProFee Coding Examples: Across Different Healthcare Specialties
- ProFee Coding vs Facility Coding: Which One affects Revenue More?
- ProFee Coding Key Guidelines in 2026
- Top ProFee Coding Mistakes Healthcare Providers Make
- How AI Is Transforming ProFee Coding
- Get ProFee Coding Right with AI
- FAQs
What Is ProFee Coding?
ProFee coding—short for professional fee coding—is the process of translating the clinical services performed by a physician or other qualified healthcare professional into billable codes for payer submission.
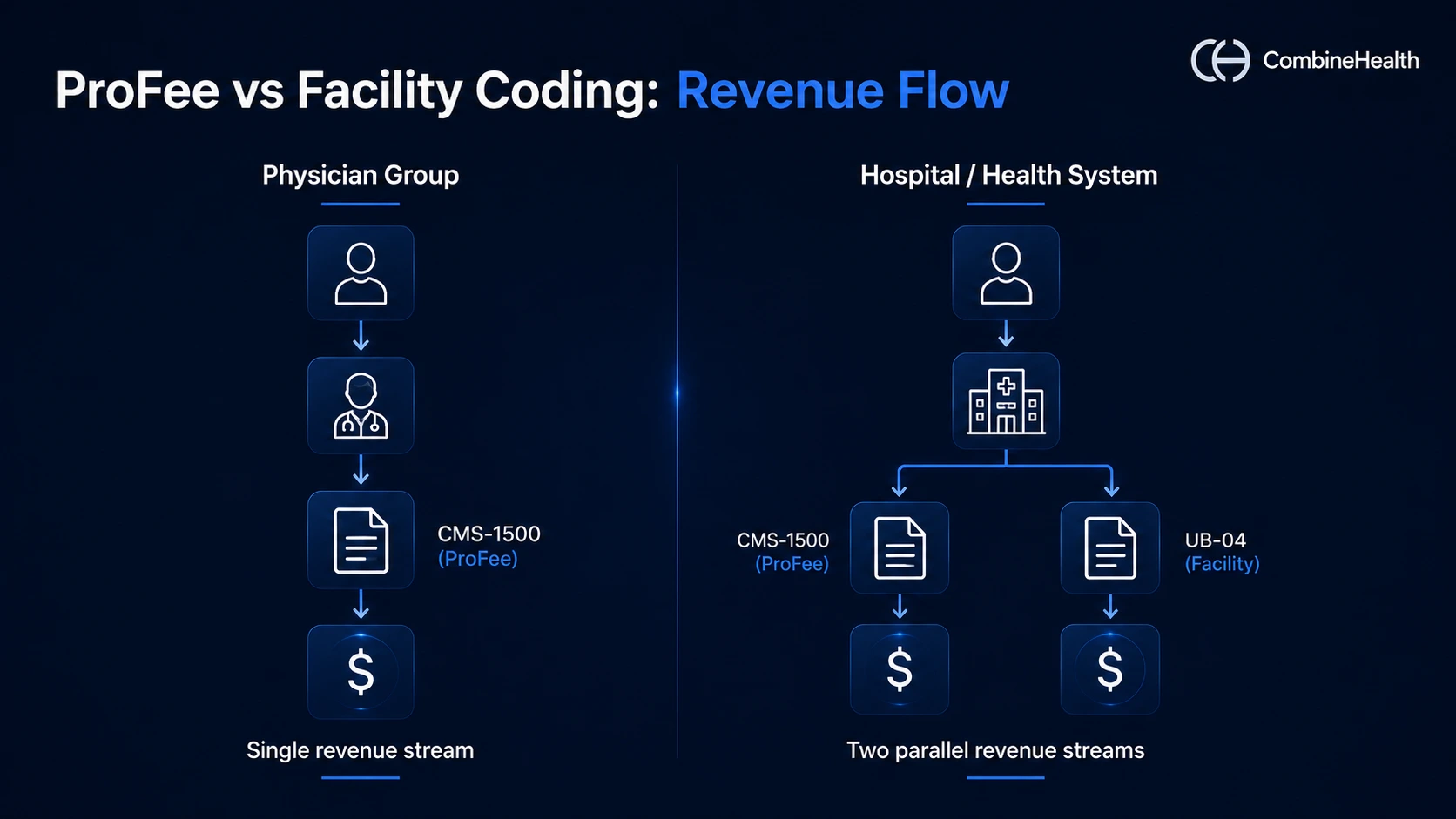
When a physician treats a patient in a hospital, two separate claims are created for the same encounter: one from the hospital (facility) and one from the physician (profee).
The "professional fee" refers specifically to the provider's work. It does not include the room, equipment, nursing staff, or supplies used during the encounter—those are captured by the facility's own claim.

The profee claim is filed on a CMS-1500 form and submitted by the physician's practice or billing team. It uses three primary code sets:
- CPT codes—describe the procedure or service performed
- ICD-10-CM codes—provide the diagnosis justifying the service
- HCPCS Level II codes—cover drugs, supplies, and non-physician services not in CPT
Reimbursement Structure and Provider Types
Reimbursement is determined by Medicare's Physician Fee Schedule. Each service gets a Relative Value Unit (RVU)—a weight reflecting the work and cost involved—multiplied by a dollar conversion factor, then adjusted for geography.
ProFee coding applies to a wide range of providers, including:
- Physicians (all specialties)
- Nurse practitioners and physician assistants
- Certified Registered Nurse Anesthetists (CRNAs)
- Radiologists and pathologists
- Hospitalists and intensivists
- Behavioral health practitioners
Any licensed provider who bills independently for professional services has a profee coding workflow—whether they're seeing patients in their own office, in a hospital outpatient department, or via telehealth.
ProFee Coding Examples: Across Different Healthcare Specialties
ProFee coding applies to every setting and specialty in physician work.
The clearest way to understand profee coding is to see what a claim actually looks like across different settings.
Office E/M ProFee Coding
Office Evaluation and Management (E/M) profee coding is the highest-volume category in most physician practices—and the one most disrupted by recent coding-rule changes.
Since the 2021 AMA guideline overhaul, office E/M codes (99202–99205 for new patients, 99211–99215 for established) are leveled by either total time spent on the visit or medical decision-making (MDM) complexity. History and physical exam no longer count toward code selection. MDM is scored across three components: problems addressed, data reviewed, and risk of complications.
Example:
An established patient sees an internist for two chronic conditions (managed hypertension and Type 2 diabetes) and one new symptom (persistent fatigue).
The physician adjusts medications and orders labs. Three problems addressed + prescription drug management + moderate risk = level-4 (99214) by MDM.
If the encounter took 35 minutes, 99214 also qualifies by time.
Recommended reading: E&M coding in 2025
ED ProFee Coding
Emergency department profee coding is one of the most nuanced settings in professional fee billing. The ED physician and the hospital each bill separately for the same visit.
The physician bills using E/M codes 99281–99285, selected based on medical decision-making (MDM) complexity. The hospital, meanwhile, bills under the Outpatient Prospective Payment System (OPPS) using Ambulatory Payment Classifications (APCs)—a completely separate methodology.
Example:
A patient presents to the ED with chest pain. The ED physician orders an ECG, interprets results, and consults cardiology.
The appropriate profee code is 99285 (high-complexity MDM).
The hospital separately bills the facility charge for the room, nursing, and equipment.
Recommended reading: Complete guide to medical coding for emergency rooms
Radiology ProFee Coding
Radiology ProFee coding runs on the split-billing model—the same imaging study generates two claims when the radiologist and the imaging facility are separate entities.
The radiologist bills the professional component (the interpretation, the report, the findings) using the radiology CPT code with modifier 26. The facility bills the technical component (equipment, technologist labor, supplies) using the same code with modifier TC. Together, they cover what would otherwise be billed as a single global service.
Example:
A radiologist reads a chest CT (CPT 71250) performed on hospital equipment. The radiologist's ProFee claim reports 71250 with modifier 26. The hospital separately bills 71250 with the modifier TC. Drop modifier 26 from the profee claim, and the entire payment routes to the facility.
Surgical ProFee Coding
Surgical ProFee coding centers on the global surgery package—a bundled payment that covers the surgeon's work before, during, and after the procedure for a set number of days.
Each surgical CPT code is assigned a global period of 0, 10, or 90 days. Within that window, the pre-op evaluation, the surgery itself, and routine post-op visits are bundled into one payment. Anything billed separately inside the global period requires a specific modifier and supporting documentation—24 for unrelated E/M, 25 for same-day separate E/M, 79 for an unrelated procedure.
Example:
A general surgeon performs a laparoscopic cholecystectomy (CPT 47562), a 90-day global procedure. The pre-op visit, the surgery, and routine post-op visits within 90 days are bundled into a single payment. If the patient returns inside that window for an unrelated UTI, the surgeon can bill that E/M visit only with modifier 24 appended.
ProFee Coding vs Facility Coding: Which One affects Revenue More?
Both profee and facility coding affect the bottom line—but they do so through completely different mechanisms.
The bigger revenue driver usually depends on the type of healthcare organization you’re looking at.
- For physician groups and clinics, profee coding is the entire revenue engine—there's no facility side.
- For hospitals and health systems, facility coding carries the heavier weight, since inpatient stays, equipment, and nursing care drive most of institutional revenue.
Understanding the distinction matters because errors in each type have different causes, different consequences, and require different prevention strategies.
Where profee coding leaks revenue: The most common profee losses are undercoding (billing a lower E/M level than documentation supports), missing the professional component modifier (-26) on split-billing claims, and failing to capture all separately billable procedures in a surgical encounter.
Where facility coding leaks revenue: Facility losses tend to involve charge capture failures—services provided but never entered—and DRG assignment errors that underpay the global hospitalization.
ProFee Coding Key Guidelines in 2026
The CY 2026 Medicare Physician Fee Schedule Final Rule (CMS-1832-F), published October 31, 2025, and effective January 1, 2026, introduced several changes that directly affect profee coding workflows and reimbursement rates.
Here are the five biggest shifts:
Two Conversion Factors—A First Under the PFS
For the first time in the history of the Physician Fee Schedule, CMS published two separate conversion factors and two RVU worksheets (RVU26A).
- Qualifying APM participants (QPs) get $33.57 (+3.77%)
- Non-QPs get $33.40 (+3.26%).
ProFee coders need to know which conversion factor applies to each rendering provider and confirm APM participation status quarterly, since the dollar gap between the two grows over time.
Efficiency Adjustment on Work RVUs
CMS finalized a -2.5% efficiency adjustment to work RVUs and intraservice time for non-time-based services. Surgeries, radiology, and most diagnostic procedures take the hit.
Exempt: E/M visits, behavioral health, maternity globals, care management, services on the Medicare telehealth list, and all 2026 new CPT codes.
For surgical and procedural claims, accurate code selection now matters more. A misassigned code that underrepresents work compounds with a lower base RVU.
Facility PE RVU Cut
Indirect practice expense (PE) RVUs allocated by work RVUs are cut by 50% in facility settings starting in 2026.
The same CPT code now pays meaningfully more in the office than in the hospital outpatient department.
Hospital-employed physicians take the hit; office-based physicians benefit. ProFee coders should be confirming place-of-service codes against actual location, especially for hybrid practices where physicians rotate between office and HOPD.
Telehealth Goes Permanent
Frequency limits on subsequent inpatient visits, subsequent nursing facility visits, and critical care consultations via telehealth are permanently removed.
Virtual direct supervision (audio-video, not audio-only) is also permanent for incident-to services and diagnostic tests, though not for procedures with 010 or 090 global periods.
ProFee documentation must specify communication mode, consent, and duration.
G2211 Expands to House Calls
HCPCS code G2211 (visit complexity add-on) now applies to home and residence E/M services (the 99341–99350 code family), not just office.
Primary care, geriatrics, and palliative care groups managing longitudinal care for homebound patients stand to gain the most from this expansion.
Also worth noting: new code 99470 (RPM patient management) carries work RVUs and is profee-billable; sibling code 99445 (RPM device supply) is facility-only.
Additional Resource:
If you’d like to learn more about this in detail, the American Society of Hematology's CY 2026 MPFS summary and Haugen Consulting's 2026 CPT updates for profee coders Q&A walk through specialty-level impacts in more detail.
Top ProFee Coding Mistakes Healthcare Providers Make
These are the errors that show up repeatedly in profee auditsand cost the most revenue:
Undercoding E/M levels
Selecting 99213 when documentation supports 99214 leaves money on the table for every affected encounter. At scale across a multi-physician practice, undercoding can represent hundreds of thousands in annual revenue loss. The fix: use MDM complexity or total provider time, whichever better reflects the encounter.
Missing modifier 26 on split-billing claims
Imaging interpretations, ECG reads, and other diagnostic services have a professional component (the read) and a technical component (the equipment). When the physician interprets but doesn't own the equipment, modifier 26 must be appended. Without it, the entire payment routes to the facility—or triggers a recoupment demand if the error is caught downstream.
Modifier -25 misuse or omission
When a physician performs both an E/M service and a procedure on the same day, Modifier -25 must be appended to the E/M code to signal a separately identifiable service. Without it, the E/M bundles into the procedure payment, and the physician receives less than earned. Conversely, using -25 without documentation of a distinct E/M assessment triggers audits.
Global surgery package errors
Each surgical CPT has a defined global period (0, 10, or 90 days). Visits within that window are bundled into the original procedure payment unless they meet specific exception criteria (modifier 24 for unrelated E/M, modifier 79 for unrelated procedure). Billing routine post-op visits without modifier awareness is a common audit trigger.
Accepting Payer Downcoding Without Challenge
Payers increasingly use AI-driven adjudication to silently downgrade billed E/M levels, which leads to a lower payment. Without active payer downcoding detection, these adjustments accumulate quietly across thousands of claims, eroding net collections without ever triggering a denial review.
Recommended reading: Common claim denial codes
How AI Is Transforming ProFee Coding
ProFee coding has historically been a manual workflow with light technology assistance. The 2026 shift is toward agentic AI in healthcare: systems that autonomously read the full encounter, assign the codes, validate them against payer policy, and route only the genuine edge cases to human reviewers.
Here’s what that looks like in practice:
- Full-encounter reading: Instead of template-driven coding from a problem list, AI agents process the entire EHR record—notes, vitals, labs, operative reports, consults, discharge summaries—and assign codes from the actual clinical narrative.
- Real-time MDM validation: For E/M codes, AI parses documentation against the 2021/2023 MDM grid in real time, flagging when documentation supports a higher level than the coder selected (or vice versa).
- Modifier intelligence: Modifiers 25, 26, 59, 57, and 50 each carry payer-specific rules. AI agents apply payer-segmented logic to flag missing or incorrect modifiers before claim submission.
- Payer policy layering: LCDs, NCDs, frequency edits, and bundling rules vary by payer. AI agents validate every code against the relevant payer's current policy, with citations.
- Human-in-the-loop for the gray zone: AI handles the 80–90% of claims that follow clear rules, then routes the ambiguous or high-risk encounters to specialty-credentialed human coders for review.
Get ProFee Coding Right with AI
ProFee coding doesn't have a simple fix.
The code sets change, payer rules shift, and documentation requirements vary by specialty, setting, and provider type. For billing teams managing hundreds of encounters a week, the margin for manual error is almost inevitable.
That's where CombineHealth's Amy AI comes in.
Amy (AI medical coding solution) is built to handle the full profee workflow, from CMS-1500 generation and eligibility verification to claim scrubbing, submission, and payment posting, across 50+ payer portals. He learns from prior denial patterns, applies payer-specific billing rules, and flags claims that need human review before they reach the clearinghouse.
For practices fighting the leaks this guide has covered—undercoding, missed modifiers, accepted downcoding, global period errors—Amy addresses each at the billing layer, before claims leave the building.
Book a demo to see what a fully automated profee billing workflow looks like in practice!
FAQs
1. What is profee coding?
ProFee coding (professional fee coding) is the process of translating a physician's clinical work into CPT, HCPCS, and ICD-10-CM codes for billing on a CMS-1500 claim form. It captures the provider's professional services separately from the facility's resource charges billed on the UB-04.
2. What are the main differences between profee coding and facility coding?
ProFee coding captures physician work (CMS-1500, CPT codes, RVU-based reimbursement). Facility coding captures institutional resources (UB-04, often APCs or DRGs). The same encounter generates both claims, reimbursed independently.
3. What is an example of profee coding?
A common example is office E/M coding: a physician bills CPT 99214 (level-4 established patient visit) on a CMS-1500 form. The claim covers only the physician's professional work—not facility costs like room, equipment, or nursing.
Recommended Reads







Related Posts
Lorem ipsum dolor sit amet, consectetur adipiscing elit. Suspendisse varius enim in eros elementum tristique. Duis cursus, mi quis viverra ornare, eros dolor interdum nulla, ut commodo diam libero vitae erat. Aenean faucibus nibh et justo cursus id rutrum lorem imperdiet. Nunc ut sem vitae risus tristique posuere.








Subscribe to newsletter - The RCM Pulse
Trusted by 200+ experts. Subscribe for curated AI and RCM insights delivered to your inbox
Let’s work together and help you get paid
Book a call with our experts and we'll show you exactly how our AI works and what ROI you can expect in your revenue cycle.
Email: info@combinehealth.ai

