The Healthcare Reimbursement Process: How Do Hospitals Get Paid
A complete guide to healthcare reimbursement, including payer types, billing workflows, reimbursement models, claim denials, and how hospitals and providers receive payment.
May 14, 2026


Key Takeaways:
• Healthcare reimbursement is the process through which providers get paid after submitting claims to insurers, government programs, or patients for medical services rendered.
• Reimbursement in healthcare depends on payer contracts, coding accuracy, documentation quality, and reimbursement models like FFS, DRGs, capitation, or value-based care.
• Different payer types — Medicare, Medicaid, commercial insurers, Medicare Advantage, and self-funded plans — follow different billing rules and payment structures.
• Hospitals, physician groups, specialty practices, and FQHCs all use different reimbursement systems based on their care settings and patient populations.
• Common reimbursement delays come from coding errors, prior authorization failures, missing documentation, eligibility issues, and denial backlogs.
• AI is increasingly used to automate coding, billing, denial prevention, appeals, eligibility checks, and reimbursement analytics across the revenue cycle.
Most people working in healthcare finance understand the stakes of reimbursement.
The CFO watching denial rates climb.
The billing manager chasing the same payer for the third time.
The coding team flagged on an audit.
Nobody needs to be convinced that getting reimbursement right matters.
What's harder is getting a clear view of how it all actually works end to end.
The system has grown complex enough that even experienced teams struggle to see it completely.
- Different payers follow different rules.
- Payment rates shift depending on the care setting.
- A claim that should have been straightforward gets denied for a reason that traces back to a documentation gap from three steps earlier in the process.
Most revenue leakage doesn't come from one big breakdown. It comes from small, recurring problems at specific points in a process that's difficult to manage as a whole.
This article breaks down how healthcare reimbursement actually works — the payment models, the payer types, how rates are determined, how the process differs across care settings, where it most commonly goes wrong, and how AI is helping close the gaps that manual workflows can't keep pace with.
On this page
- What is Healthcare Reimbursement?
- How Does Reimbursement in Healthcare Work
- Types of Payers for Health Claims
- How Does Reimbursement Work in Different Healthcare Settings?
- Types of Reimbursement Models in Healthcare
- How Hospital Reimbursement Rates Are Determined
- How Payer Mix Shapes Overall Healthcare Revenue
- Issues Causing Delays in Healthcare Reimbursement
- How AI helps Improve the Healthcare Reimbursement Process
- Start Closing the Reimbursement Gaps in Your Healthcare Revenue Cycle
- FAQs
- How does insurance reimbursement work in healthcare?
- What are the common payment methods for healthcare services?
- What are reimbursement methodologies in healthcare?
- What are the different reimbursement models used in healthcare?
- Who typically reimburses healthcare providers for their services?
- What are third-party payers in healthcare?
- Can you explain how hospital reimbursement rates are determined?
- What is Medicare reimbursement?
- What is Medicaid reimbursement?
- What are the main payer types for health claims?
- What are the main issues causing delays in healthcare reimbursement?
What is Healthcare Reimbursement?
Healthcare reimbursement is the process through which hospitals, physician groups, federally qualified health centers, and other providers recover payment from insurance companies for the clinical services they deliver.
Healthcare reimbursement is how providers get paid for the care they deliver. When a hospital, physician group, or federally qualified health center submits a claim to an insurance company, reimbursement is the process that determines how much of that claim will actually be paid.
What distinguishes healthcare reimbursement from conventional billing is that the payment amount is rarely determined by what the provider charges. It's determined by:
- Contracted fee schedules negotiated between the provider and each payer
- Government-set base rates
A provider’s chargemaster rate may serve as the starting point, but the actual allowed amount is shaped by payer contracts, regulatory guidelines, patient eligibility, and how accurately the claim was coded and submitted.
What is a Chargemaster?
A chargemaster is a hospital’s comprehensive internal pricing list for every service, procedure, medication, supply, and piece of equipment it provides.
Every hospital maintains its own chargemaster, and it acts as the starting point for generating patient bills and insurance claims.
How Does Reimbursement in Healthcare Work
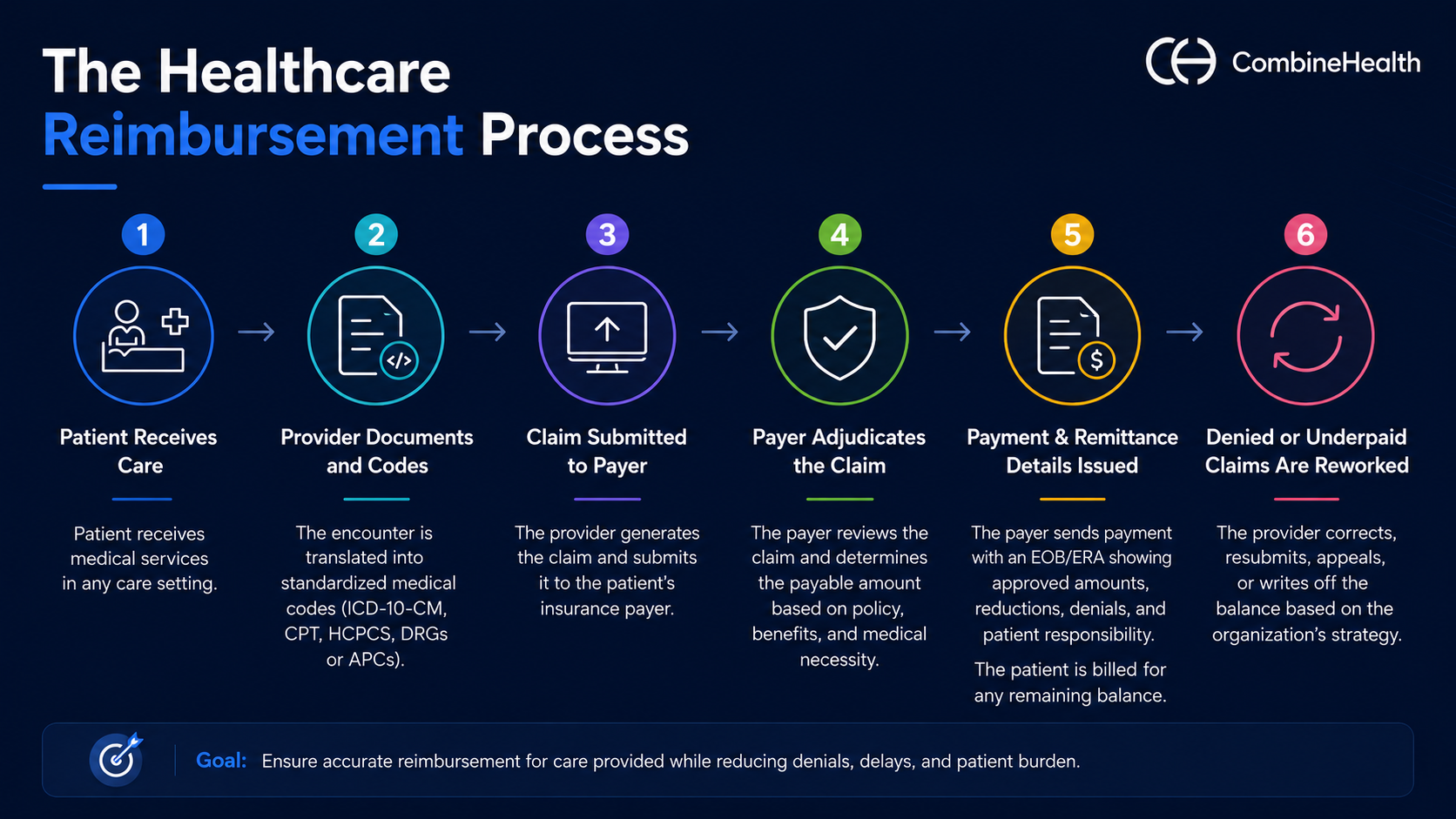
Healthcare reimbursement typically follows a multi-step process that involves the following steps:
1. The patient receives care: This could include inpatient treatment, outpatient services, emergency department visits, ambulatory surgery, clinic appointments, or diagnostic testing.
2. The provider documents and codes the encounter: The clinical encounter is translated into standardized medical codes using ICD-10-CM, CPT, and HCPCS codes. Hospitals may also use DRGs or APCs depending on the care setting and reimbursement model.
3. The claim is submitted to the payer: Once coding is complete, the provider generates a claim and submits it to the patient’s insurance payer. This may include Medicare, Medicaid, commercial insurers, Medicare Advantage plans, managed Medicaid organizations, or self-funded employer plans.
4. The payer adjudicates the claim: The insurance company reviews the claim against its reimbursement policies, fee schedules, benefit structures, prior authorization requirements, and medical necessity guidelines to determine how much will be paid.
5. Payment and remittance details are issued: The payer sends reimbursement along with an explanation of benefits (EOB) or electronic remittance advice (ERA) that outlines approved amounts, reductions, denials, and patient responsibility. Remaining balances such as deductibles, co-pays, or co-insurance are billed to the patient.
6. Denied or underpaid claims are reworked: If the claim is denied, partially paid, or rejected, the provider may correct and resubmit the claim, file an appeal, submit supporting documentation, or write off the balance depending on the organization’s denial management strategy.
Types of Payers for Health Claims
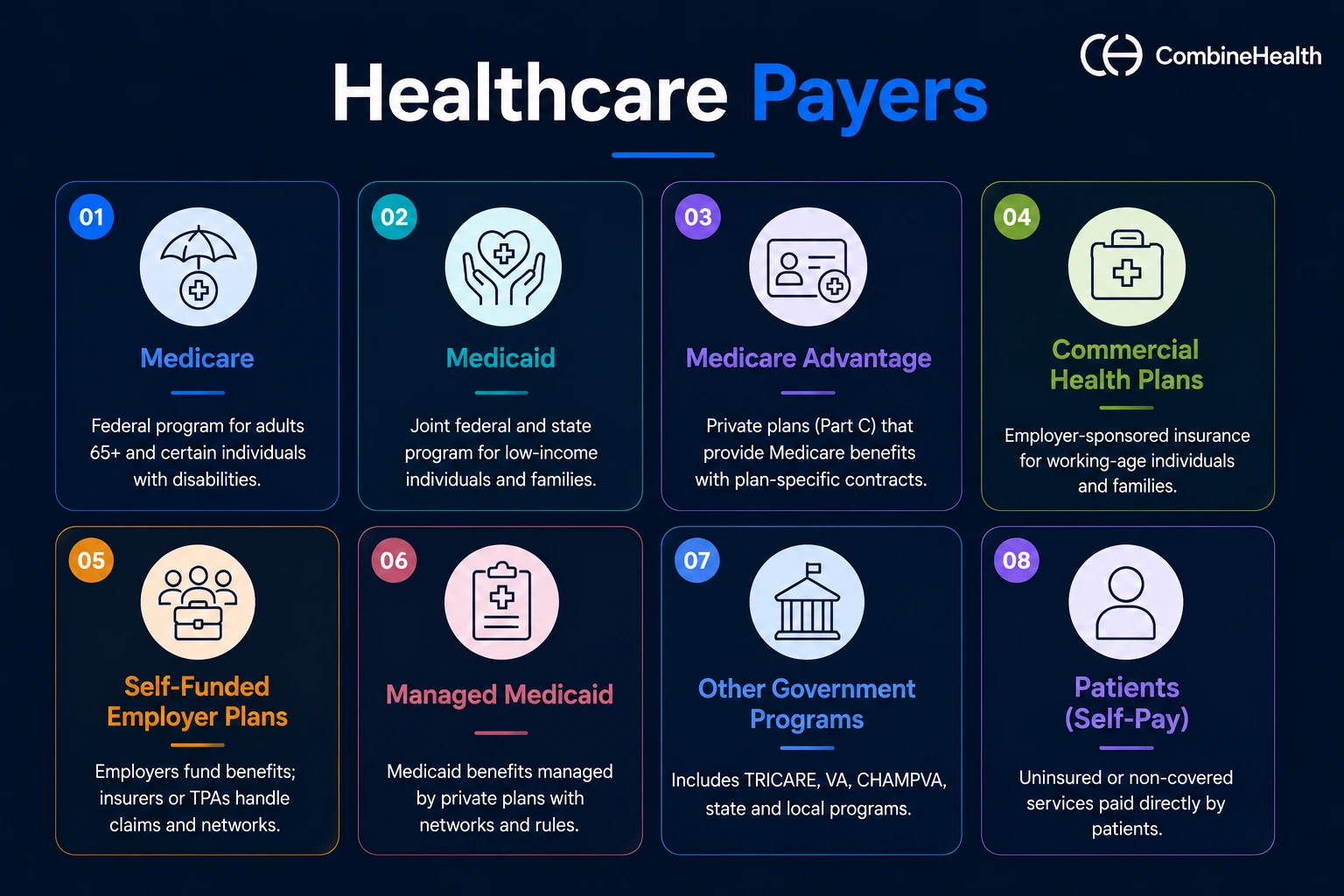
A single hospital or physician group may submit claims to multiple payer types every day, each with its own reimbursement rules, documentation requirements, and fee schedules. This typically involves payers like:
Medicare
Medicare is the federal health insurance program administered by the Centers for Medicare & Medicaid Services for adults 65 and older, and younger individuals with certain disabilities or end-stage renal disease. It’s the largest payer for many hospitals and physician groups and often sets the baseline other payers negotiate around.
Medicare uses standardized reimbursement systems, including:
- Inpatient Prospective Payment System (IPPS) for hospital stays
- Physician Fee Schedule (PFS) for professional services
Medicare reimbursement is highly structured and non-negotiable. There’s no contract-based rate negotiation. Medicare pays based on its established fee schedules, and providers are expected to:
- Submit claims accurately
- Meet documentation requirements
- Follow coding guidelines
- Comply with coverage policies such as Local Coverage Determinations (LCDs), which define when services are considered medically necessary
Medicaid
Medicaid is a government-funded health insurance program for low-income adults, children, pregnant women, and individuals with disabilities. Unlike Medicare, Medicaid is jointly funded by federal and state governments, which means reimbursement rules and payment structures can vary significantly across states.
For many safety-net hospitals and federally qualified health centers (FQHCs), Medicaid represents a large share of total patient volume, especially in states that expanded Medicaid under the Affordable Care Act.
Medicaid reimbursement is often associated with:
- Lower payment rates than Medicare
- State-specific coverage and billing rules
- Higher administrative complexity
- Tighter operating margins for providers
Medicare Advantage
Medicare Advantage, also known as Medicare Part C, allows patients to receive Medicare-covered benefits through private insurance companies instead of traditional Medicare.
While the patient population is still Medicare-eligible, the reimbursement process works very differently for providers.
Unlike traditional Medicare, Medicare Advantage plans operate with their own:
- Provider networks
- Payer-specific claims workflows
- Separate reimbursement contracts
- Unique prior authorization requirements
Payment rates are negotiated directly with each plan, which means reimbursement can vary significantly across insurers and markets.
Commercial Health Plans
Commercial health plans primarily cover working-age individuals and their dependents through employer-sponsored insurance. This category includes large national insurers such as UnitedHealthcare, Elevance Health, Aetna, and Cigna, along with regional and Blue Cross Blue Shield plans.
Unlike Medicare or Medicaid, reimbursement rates for commercial plans are contractually negotiated between providers and insurers, with contracts typically revisited every one to three years.
Commercial reimbursement is often associated with:
- Higher payment rates than government payers
- Contract-based fee schedules
- Payer-specific reimbursement policies
- Greater variation in reimbursement across markets and specialties
Self-Funded Employer Plans
Many large employers don’t purchase traditional insurance coverage from a health plan. Instead, they self-fund their employee health benefits, meaning the employer takes on the financial risk for healthcare claims while partnering with an insurer or third-party administrator (TPA) to handle claims processing and network administration.
From a provider’s perspective, the workflow may look similar to a commercial payer relationship since claims still move through the insurer’s systems. But the underlying plan rules and coverage decisions are ultimately determined by the employer.
Self-funded plans are typically associated with:
- Employer-funded healthcare coverage
- Claims administration through insurers or TPAs
- Customized benefit structures
- Plan-specific reimbursement policies
These plans are generally governed by Employee Retirement Income Security Act of 1974 (ERISA) rather than state insurance regulations
Managed Medicaid
In many states, Medicaid benefits are administered through private managed care organizations (MCOs) instead of traditional fee-for-service Medicaid programs. That means providers typically contract with managed care plans rather than billing the state Medicaid agency directly.
Operationally, managed Medicaid plans often resemble commercial insurers. They maintain:
- Provider networks
- Prior authorization requirements
- Utilization management policies
- Payer-specific claims workflows
However, reimbursement rates generally remain at or near traditional Medicaid levels.
Patients
Patients are also an important part of the reimbursement process and increasingly, a growing source of provider revenue responsibility.
After insurance pays its portion of the claim, the remaining balance becomes the patient’s responsibility. This can include:
- Deductibles
- Co-insurance
- Co-pays
- Non-covered services
As high-deductible health plans have become more common, patient financial responsibility has increased significantly across healthcare organizations.
How Does Reimbursement Work in Different Healthcare Settings?
Medium-Large Hospitals
Hospital reimbursement is built around large-scale facility payment systems designed to account for high operating costs, complex care delivery, and large patient volumes.
For Medicare patients, inpatient hospital stays are typically reimbursed through Diagnosis-Related Groups (DRGs), where the hospital receives a fixed payment based on the patient’s:
- Diagnosis
- Severity and complexity of the case
- Procedures performed
- Hospital-specific factors such as teaching status or geographic location
Outpatient hospital services are generally reimbursed through Ambulatory Payment Classifications (APCs) under the Outpatient Prospective Payment System (OPPS), while physician services are billed separately through the Physician Fee Schedule.
MSOs and Physician Groups
For MSOs and physician groups, reimbursement is tied much more directly to professional fee schedules and the accuracy of individual claim-level coding.
Under Medicare, physician reimbursement is based on the Physician Fee Schedule and calculated using Relative Value Units (RVUs). Each service or procedure is assigned:
- A physician work value
- A practice expense value
- A malpractice expense value
Those RVUs are then adjusted geographically and multiplied by a conversion factor to determine the final reimbursement amount.
Commercial payers may:
- Benchmark reimbursement against Medicare rates
- Reimburse at a percentage of Medicare
- Use their own negotiated fee schedules depending on the contract structure
Key revenue drivers include:
- Accurate E/M level selection
- Procedure coding precision
- Correct modifier usage
- Documentation quality
- Prior authorization management
- Denial prevention
Specialty Groups
Specialty groups operate within the same physician fee schedule structure as broader physician practices, but reimbursement is shaped much more heavily by specialty-specific procedures, service intensity, and payer policies.
Procedure-heavy specialties such as orthopedics, cardiology, gastroenterology, and pain management generate a large portion of revenue from:
- Surgical and procedural codes
- Implants and device-related billing
- Imaging and ancillary services
- High-value treatment encounters
In these specialties, reimbursement often depends heavily on:
- Bundled payment terms
- Carve-outs for high-cost procedures
- Implant reimbursement policies
- Payer-specific authorization requirements
FQHCs
FQHCs operate under a fundamentally different reimbursement structure than hospitals or traditional physician groups.
Instead of billing primarily on a line-by-line fee-for-service basis, Medicare and Medicaid typically reimburse FQHCs through prospective payment systems (PPS) built around per-visit or per-encounter rates.
Under Medicare, qualifying visits are reimbursed through an all-inclusive bundled payment adjusted for geographic factors. Medicaid programs also establish PPS encounter rates, although states may use alternative payment methodologies within federal guidelines.
For FQHCs, reimbursement performance depends heavily on:
- Correctly qualifying encounters
- Capturing every eligible visit
- Managing payer-specific billing rules
- Reconciling wrap-around payments accurately
When FQHCs contract with Medicaid managed care organizations or Medicare Advantage plans, those plans may reimburse below the PPS-equivalent amount. In those cases, supplemental wrap-around payments are used to bridge the gap between managed care reimbursement and the federally required PPS rate.
Types of Reimbursement Models in Healthcare
Over the decades, the industry has developed several distinct payment models — each with a different logic for how much gets paid, when, and based on what.
Traditional Fee‑for‑Service (FFS)
Fee-for-service is the most traditional reimbursement model in healthcare.
Under this structure, the provider:
- Delivers a service
- Submits a claim for that service
- Receives payment based on a predefined fee schedule
Every office visit, procedure, imaging study, or lab test is billed and reimbursed separately.
Centers for Medicare & Medicaid Services Medicare’s Physician Fee Schedule is one of the most widely used examples of fee-for-service reimbursement, and many commercial payers structure their reimbursement rates as a percentage of Medicare rates.
The model is operationally straightforward because providers generally know:
- What was billed
- What the contracted reimbursement rate is
- How payment will be calculated
The challenge is that fee-for-service primarily rewards volume. Payment is tied to the number of services delivered rather than whether patient outcomes improved or costs were reduced over time.
Recommended Reading: Fee for service vs value-based care models
Prospective Payment Systems
Hospitals are often reimbursed through prospective payment systems, where the payment amount is determined in advance based on the patient’s diagnosis and clinical complexity rather than the exact number of services delivered.
For inpatient care, Medicare assigns each hospitalization to a Diagnosis-Related Group (DRG). The hospital then receives a fixed bundled payment for the entire stay.
That payment is influenced by factors such as:
- Primary diagnosis
- Procedures performed
- Patient severity
- Hospital characteristics
Under this model hospitals retain savings if care costs less than the DRG payment, but absorb financial losses if the cost of care exceeds reimbursement.
Capitation
Under capitation, providers receive a fixed payment per patient, per month — commonly referred to as PMPM (per member per month) reimbursement.
The provider receives that payment regardless of how many services the patient actually uses during the coverage period.
This model shifts more financial risk to the provider:
- If patients require less care, the provider retains the surplus
- If care costs exceed the fixed payment, the provider absorbs the loss
Capitation is commonly used in:
- Medicare Advantage plans
- Managed Medicaid arrangements
- Some value-based care contracts
Bundled and Episode‑Based Payments
Bundled payments combine multiple services related to a specific episode of care into a single reimbursement amount.
For example, a bundled payment for a hip replacement may include:
- The surgery itself
- Hospital services
- Anesthesia
- Rehabilitation
- Certain post-acute care costs within a defined timeframe
Compared to traditional fee-for-service, bundled payment arrangements require much more coordination because reimbursement must often be distributed across multiple providers and organizations involved in the patient’s care.
Shared Savings and Value-Based Models
Shared savings models typically operate on top of traditional fee-for-service reimbursement.
Providers continue billing for services normally, but total healthcare spending for a defined patient population is measured against a benchmark over time.
The providers may receive a portion of the savings generated, if they:
- Reduce total costs
- Meet quality benchmarks
- Improve care outcomes
More advanced value-based arrangements may also include two-sided risk models, where providers share responsibility for financial losses if spending exceeds target benchmarks.
These models are increasingly common in:
- Accountable Care Organizations (ACOs)
- Medicare Advantage
- Population health initiatives
How Hospital Reimbursement Rates Are Determined
They're the product of two parallel tracks — government-mandated payment systems that apply to Medicare and Medicaid, and contract negotiations with commercial payers that produce individually negotiated rates.
How Medicare Sets Hospital Rates
Medicare reimbursement rates are not negotiated individually with hospitals. Instead, they are established through federal payment systems updated annually through CMS rulemaking.
Most inpatient hospital stays are reimbursed under the Inpatient Prospective Payment System (IPPS), where each admission is assigned to a Diagnosis-Related Group (DRG) based on:
- Primary and secondary diagnoses
- Procedures performed
- Patient severity
- Age
- Discharge status
Medicare also adjusts reimbursement based on factors such as:
- Geographic wage differences
- Teaching hospital status
- Disproportionate share hospital (DSH) adjustments
- Quality reporting performance
How Medicaid Rates Are Set
Medicaid reimbursement rates are established by individual states within federal guidelines, which creates significant variation across markets.
Most states use some form of prospective payment methodology, including:
- DRG-based inpatient reimbursement
- APC-based outpatient reimbursement
- State-specific fee schedules
Compared to Medicare and commercial plans, Medicaid reimbursement rates are typically lower and may not fully cover the actual cost of care.
States may also issue supplemental payments for hospitals serving large Medicaid and uninsured populations through:
- Disproportionate share hospital (DSH) payments
- Upper payment limit (UPL) programs
How Commercial Rates Are Negotiated
Commercial reimbursement rates are determined through contract negotiations between hospitals and private insurers.
Contracts may define reimbursement as:
- A percentage of Medicare rates
- Hospital-specific fee schedules
- Case rates
- Per-diem payment structures for certain service lines
A hospital’s negotiating leverage is often influenced by:
- Market share
- Specialty service availability
- Patient volume
- Geographic competition
- Network importance to the payer
How Payer Mix Shapes Overall Healthcare Revenue
Because different payer types reimburse at very different rate levels, payer mix has a major impact on hospital financial performance.
Hospitals with larger shares of Medicaid patients, Medicare beneficiaries and uninsured populations often generate lower reimbursement per case than hospitals with stronger commercial payer mixes.
Even when patient volume remains stable, changes in payer mix can significantly affect:
- Net revenue
- Operating margins
- Overall financial sustainability
Issues Causing Delays in Healthcare Reimbursement
Most reimbursement delays don't trace back to a single catastrophic failure. They trace back to small, recurring breakdowns at specific points in the revenue cycle — problems that are individually manageable but collectively keep cash from arriving on time, or from arriving at all.
Eligibility and Coverage Verification Gaps
When patient eligibility isn’t verified correctly before the visit — or when details like deductibles, co-pays, secondary coverage, or prior authorization requirements are missed — claims are built on incomplete information.
That often leads to:
- Eligibility denials
- Billing the wrong payer
- Coverage-related claim rejections
- Retroactive payment corrections

Prior Authorization Failures
Prior authorization is one of the biggest administrative bottlenecks in healthcare reimbursement.
The claim may be denied regardless of whether the treatment itself was clinically appropriate, if a required authorization is:
- Missing
- Expired
- Incomplete
- Doesn’t match the service ultimately delivered
The challenge is that prior authorization requirements vary significantly by payer, change frequently, and often aren't communicated clearly.
A procedure that doesn't require authorization from one commercial plan may require it from a Medicare Advantage plan covering a patient in the same practice.
Coding Errors and Inaccuracies
Medical coding directly determines how a payer interprets and reimburses a claim.
Even small coding mistakes can trigger:
- Claim denials
- Underpayments
- Compliance risk
- Manual rework
Common examples include:
- Incorrect diagnosis codes
- Missing modifiers
- Bundling violations
- E/M levels that don’t match the documented complexity of care
Incomplete or Insufficient Documentation
Coding accuracy depends heavily on clinical documentation quality.
The claim becomes vulnerable to denials, downcoding, or post-payment audits, if provider notes:
- Lack specificity
- Fail to support medical necessity
- Don’t fully capture patient complexity
This is especially important in inpatient settings where DRG reimbursement depends on capturing all relevant diagnoses and complications accurately.
Recommended Reading: Common causes of payer downcoding
Claim Submission Errors
Some claims never make it into the payer’s adjudication system at all.
Payers can reject the claim before processing begins if any of the following information is incorrect or missing:
- Wrong patient identifiers
- Invalid payer IDs
- Missing provider details
- Duplicate submissions
Denial Backlogs and Slow Appeals
Denials are common across healthcare reimbursement, but the bigger challenge is often managing them at scale.
Many organizations recover a large percentage of denied claims, but only if appeals are:
- Worked quickly
- Prioritized correctly
- Supported with payer-specific documentation
Payer-Side Adjudication Delays
Not every reimbursement delay originates with the provider.
Payers themselves may delay claim adjudication due to:
- Medical necessity reviews
- Coordination of benefits issues
- Contract disputes
- Manual review processes for complex claims
Some payer categories, particularly Medicare Advantage plans, are often associated with longer authorization and adjudication timelines compared to traditional Medicare.
How AI helps Improve the Healthcare Reimbursement Process
Healthcare reimbursement involves thousands of repetitive, rules-driven decisions across coding, billing, authorizations, denials, and documentation. AI is increasingly being used to automate those workflows, reduce administrative friction, and identify reimbursement risks earlier in the revenue cycle.
Here’s how:
Coding Automation
AI-powered coding systems analyze clinical documentation and assign:
- ICD-10 diagnosis codes
- CPT and HCPCS procedure codes
- E/M levels based on the documented encounter
Straightforward encounters can often be coded autonomously, while more complex charts are routed to human coders with:
- Suggested codes
- Supporting rationale
- Documentation references
Eligibility and Prior Authorization
AI can automate eligibility verification and prior authorization workflows by checking:
- Active coverage
- Payer requirements
- Authorization status
- Patient financial responsibility in real time across payer systems
Instead of discovering coverage problems after claim submission, organizations can identify issues before the patient encounter occurs.
Denial Prevention
Traditional denial management is reactive—the claim is denied first, then teams work to recover payment.
AI shifts part of that process upstream by analyzing:
- Historical denial trends
- Payer-specific billing behavior
- Medical necessity policies
- Claim-level risk indicators before submission
Claims that are likely to trigger denials can be flagged for correction proactively.
This is important because preventing a denial is usually far less expensive than reworking the claim, filing appeals, or extending the reimbursement timeline by weeks or months.
Denial Management and Appeals
When denials do occur, AI can help prioritize and streamline the recovery process.
AI-driven denial management systems can automatically categorize denials by:
- Payer
- Denial reason
- Dollar value
- Aging
- Filing deadlines
That allows teams to focus first on the claims with the highest financial impact.
For claim appeals workflows, AI can assist by:
- Drafting payer-specific appeal letters
- Pulling supporting clinical documentation
- Referencing coverage policies
- Organizing medical necessity evidence
Beyond individual denials, AI is also useful for identifying systemic denial patterns.
Example:
If the same denial reason repeatedly appears for the same payer, procedure, or specialty, the system can surface the root cause much earlier — whether it originates in coding, documentation, authorization, or registration workflows.
Recommended Reading: A compilation of 9 best AI appeals solutions for healthcare RCM teams
Analytics and Forecasting
AI-driven analytics platforms can process large volumes of revenue cycle data and convert them into operational and financial insights.
That includes analyzing:
- Denial rates
- A/R aging
- Payer turnaround times
- Appeal success rates
- Reimbursement trends across payer categories
Predictive forecasting models can also help finance leaders estimate:
- Expected collections
- Reimbursement delays
- Cash flow trends
- Payer performance patterns based on historical data
Clinical Documentation
AI-powered scribing and documentation tools can generate structured clinical notes from physician-patient conversations in real time.
Improved documentation quality helps support:
- Coding accuracy
- DRG assignment precision
- Medical necessity validation
- Cleaner claim submission
It also reduces:
- Physician documentation burden
- Coding clarification queries
- Delays between patient care and claim generation
Start Closing the Reimbursement Gaps in Your Healthcare Revenue Cycle
Healthcare reimbursement has never been simple. But the gap between what providers bill and what they actually collect has grown wide enough that managing it manually, with disconnected tools and reactive workflows, is no longer a sustainable strategy.
Closing that gap requires more than working harder on individual claims. It requires visibility across the full revenue cycle and the ability to act on patterns before they become write-offs.
That's what CombineHealth is built to do. A coordinated AI workforce that handles coding, billing, eligibility verification, denial management, appeals, and analytics — sharing context across every step so revenue stops slipping through the handoffs.
If your organization is seeing denial rates climb, A/R days stretch, or collections falling short of contracted rates, the place to start is a conversation.
Book a demo with CombineHealth and see what a coordinated AI revenue cycle looks like in practice.
FAQs
How does insurance reimbursement work in healthcare?
After treatment, providers submit a claim to the patient’s insurer. The payer reviews medical codes, coverage rules, and documentation before approving, reducing, or denying payment. Once processed, the provider receives reimbursement based on the patient’s plan and contracted rates.
What are the common payment methods for healthcare services?
Common payment methods include private insurance payments, Medicare, Medicaid, patient self-pay, employer-sponsored health plans, and value-based reimbursement arrangements. Payments may be made through fee-for-service, bundled payments, or capitation models.
What are reimbursement methodologies in healthcare?
Reimbursement methodologies are the formulas or approaches payers use to determine provider payments. These include fee-for-service, prospective payment systems, capitation, bundled payments, and value-based reimbursement tied to quality and outcomes.
What are the different reimbursement models used in healthcare?
Major healthcare reimbursement models include fee-for-service (FFS), capitation, bundled payments, value-based care, pay-for-performance, and accountable care organization (ACO) models. Each model balances cost control, quality, and provider incentives differently.
Who typically reimburses healthcare providers for their services?
Healthcare providers are typically reimbursed by private insurance companies, government payers like Medicare and Medicaid, workers’ compensation programs, employer-sponsored health plans, and patients through out-of-pocket payments.
What are third-party payers in healthcare?
Third-party payers are organizations that pay healthcare claims on behalf of patients. These include private insurance companies, Medicare, Medicaid, TRICARE, and employer-sponsored health plans.
Can you explain how hospital reimbursement rates are determined?
Hospital reimbursement rates are based on payer contracts, diagnosis codes, procedure complexity, geographic adjustments, patient demographics, and government payment formulas such as DRGs for inpatient services.
What is Medicare reimbursement?
Medicare reimbursement refers to payments made by the federal Medicare program to healthcare providers for covered medical services. Rates are determined using CMS fee schedules, DRG systems, and value-based payment adjustments.
What is Medicaid reimbursement?
Medicaid reimbursement is the payment healthcare providers receive for treating Medicaid beneficiaries. Rates are set jointly by state and federal governments and are usually lower than private insurance reimbursement rates.
What are the main payer types for health claims?
Major payer types include commercial/private insurance, Medicare, Medicaid, workers’ compensation, TRICARE, self-pay patients, and managed care organizations like HMOs and PPOs.
What are the main issues causing delays in healthcare reimbursement?
Common reimbursement delays include coding errors, missing documentation, prior authorization issues, eligibility problems, claim denials, payer policy changes, and manual billing workflows. Staffing shortages and payer-specific rules also contribute to delays.
Recommended Reads







Related Posts
Lorem ipsum dolor sit amet, consectetur adipiscing elit. Suspendisse varius enim in eros elementum tristique. Duis cursus, mi quis viverra ornare, eros dolor interdum nulla, ut commodo diam libero vitae erat. Aenean faucibus nibh et justo cursus id rutrum lorem imperdiet. Nunc ut sem vitae risus tristique posuere.








Subscribe to newsletter - The RCM Pulse
Trusted by 200+ experts. Subscribe for curated AI and RCM insights delivered to your inbox
Let’s work together and help you get paid
Book a call with our experts and we'll show you exactly how our AI works and what ROI you can expect in your revenue cycle.
Email: info@combinehealth.ai

